Published on 22 December 2025 Hip surgery
Implanting a hip prosthesis in coxopathy with normal radiographs
The most common procedure in hip surgery is primary total hip replacement for advanced hip osteoarthritis. In typical cases, the surgical indication is straightforward when a patient presents with progressive coxofemoral pain resistant to medical treatment, associated with joint stiffness and radiographic signs of joint degeneration. When radiographs show advanced osteoarthritis or significant femoral head necrosis, proposing prosthetic implantation is logical.

When radiographs are normal despite pain
In some cases, patients present with mechanical hip pain despite perfectly normal radiographs.
The typical scenario involves a 50-year-old woman with mechanical and positional groin pain, limiting daily activities, walking, and sports.
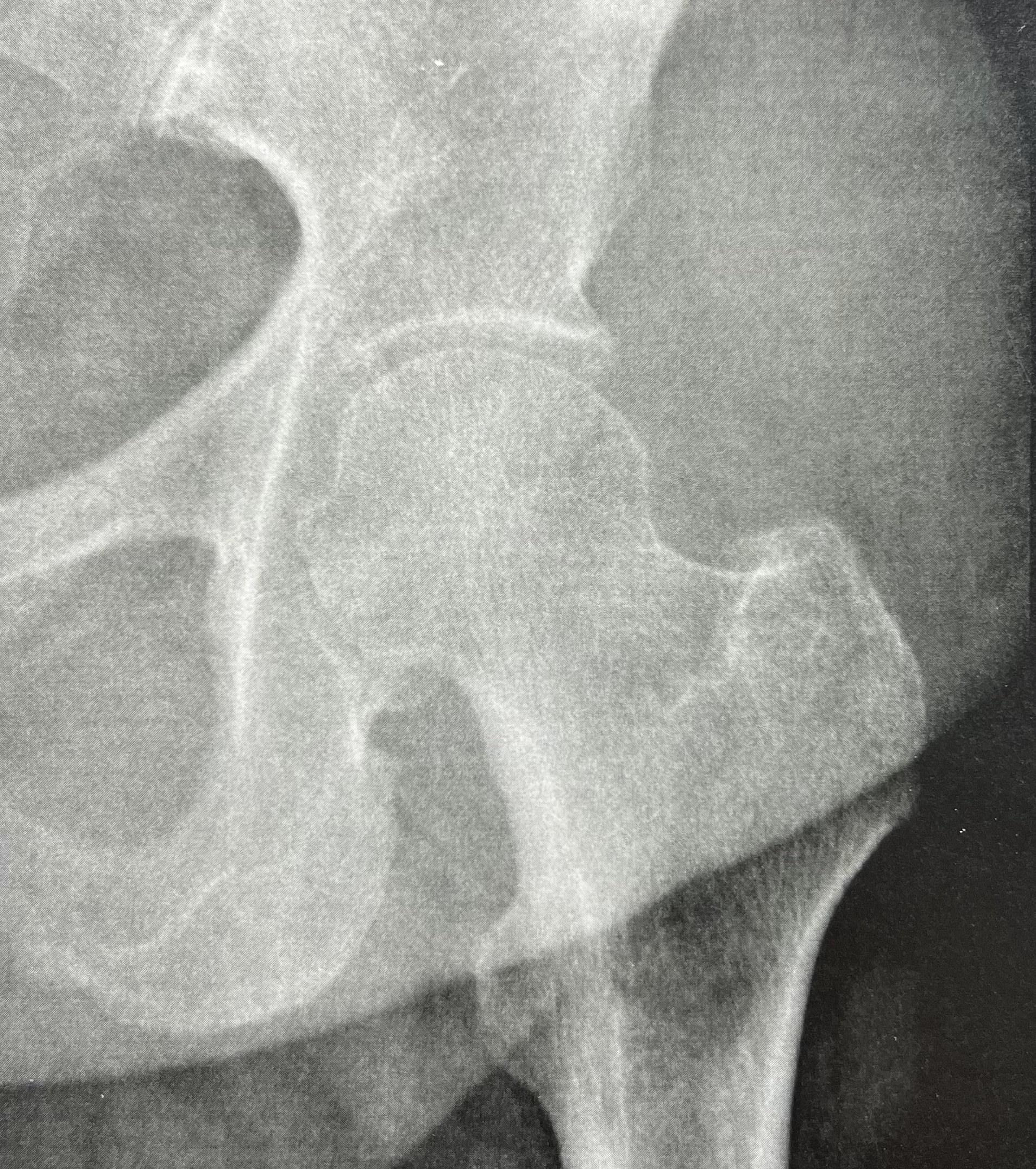
When hip radiographs are strictly normal (no joint space narrowing, no osteophytes, no subchondral cysts, and no signs of osteoarthritis ) treatment is often limited to analgesics, anti-inflammatory drugs, and injections, and any surgical option is usually ruled out.
In certain cases, however, this approach represents a strategic error, as some cartilage lesions with normal radiographs are resistant to medical treatment.
The decisive contribution of cross-sectional imaging
Cross-sectional imaging provides essential diagnostic information.
The role of hip mri
An MRI focused on the coxofemoral joint may reveal:
- joint effusion
- advanced chondropathy
- subchondral bone marrow edema in the weight-bearing zone, sometimes bipolar
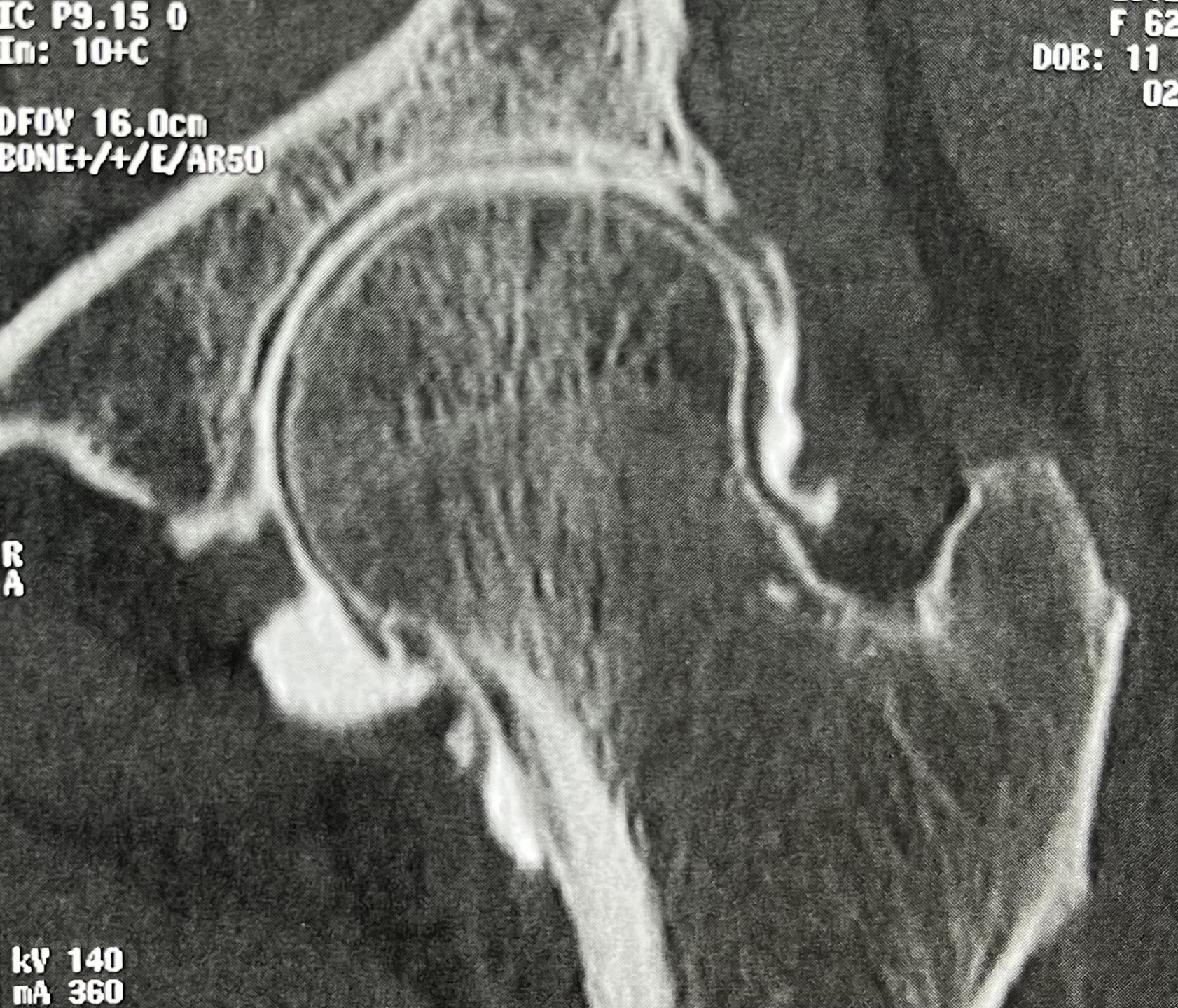
The value of CT arthrography
CT arthrography allows precise visualization of cartilage integrity and may demonstrate deep and extensive femoral chondropathy (grade IV), confirming severe joint suffering.
In some cases, the chondropathy is bipolar, affecting both femoral and acetabular cartilage.
Thus, severe and extensive chondropathy may exist despite normal radiographs.
Clinical examination: an essential step
During consultation, physical examination evaluates passive hip range of motion in all planes. Marked pain is often elicited during coxopathy tests, particularly the FABER test and the FADIR test.
A complete neurological examination is mandatory to rule out radiculopathy, sensorimotor deficits, or absent reflexes. Abdominal wall hernias and all sources of extra-articular pain must also be excluded.
Medical management of cartilage lesions with normal radiographs
In cases of severe chondropathy with normal radiographs, treatment primarily relies on joint preservation, avoiding high-impact sports and favoring gentle, regular, low-load activities such as cycling and swimming.
Medical treatment includes:
- analgesics tailored to pain intensity
- nonsteroidal anti-inflammatory drugs administered intermittently
In some cases, intra-articular injections can be highly effective (hyaluronic acid, corticosteroid, PRP).
When should a hip prosthesis be considered despite normal radiographs?
When well-conducted medical treatment fails, hip replacement may be indicated.
In such situations, priority should be given to:
- a muscle-sparing surgical technique (direct anterior approach)
- three-dimensional CT-based planning, essential for precise analysis of coxofemoral morphology
When implanting a prosthesis for coxopathy with normal radiographs, it is crucial not to alter joint anatomy, using accurate planning, rigorous surgical technique, and, whenever possible, a custom-made implant.
Outcomes and limitations of prosthetic implantation
When severe, extensive chondropathy is present and consistent with the pain presentation, total hip replacement yields excellent results, allowing full return to unrestricted activities.
Conversely, when the radioclinical picture lacks coherence—atypical, diffuse pain associated with only mild chondropathy and no objective signs of joint suffering—the prognosis is uncertain and the risk of diagnostic error is significant.
In such cases, a preoperative anesthetic test is recommended to guide the decision toward either prosthetic implantation or surgical abstention.
Surgical abstention can sometimes be the most appropriate and beneficial decision.
